
- Overcoming the autoimmune attack in T1D is a vital part of a Practical Cure.
- There are two major research pathways:
- Hiding the beta cells from the immune system (2 main tactical approaches).
- Stopping the attack at its root (5 main tactical approaches).
- These approaches have been or are being tested today in human clinical trials.
- Any ‘forced’ change to the immune system may also present significant collateral risks that need to be well understood before going to market.
April 9, 2026
This report outlines the key pathways being explored to protect insulin-producing cells from the autoimmune attack in T1D. We hope this summary overview provides a straightforward set of definitions and a simple structure for understanding and discussing a very important but scientifically complex topic.
Type 1 diabetes (T1D) occurs when the immune system mistakenly attacks and destroys its insulin-producing beta cells. Though there are theories, the exact reason why these cells are mistaken for enemies is unknown.
Any Practical Cure for T1D must provide both a ready supply of insulin-producing beta cells and a way to protect those cells from the autoimmune attack. Previously, JDCA wrote an overview of cell supply pathways. This report focuses specifically on cell protection pathways.
To date, the only proven long-term cell protection method is chronic, full-body immunosuppression, which is the standard of care for protecting transplanted organs and tissues. This approach reduces the effectiveness of one’s entire immune system in fighting disease and infection, increasing the risk of infection, cancer, toxicity, and damage to transplanted organs.
A Practical Cure must provide an alternative to full-body immunosuppression without dire side effects or risks. The pathways discussed in this report are the potential alternatives.
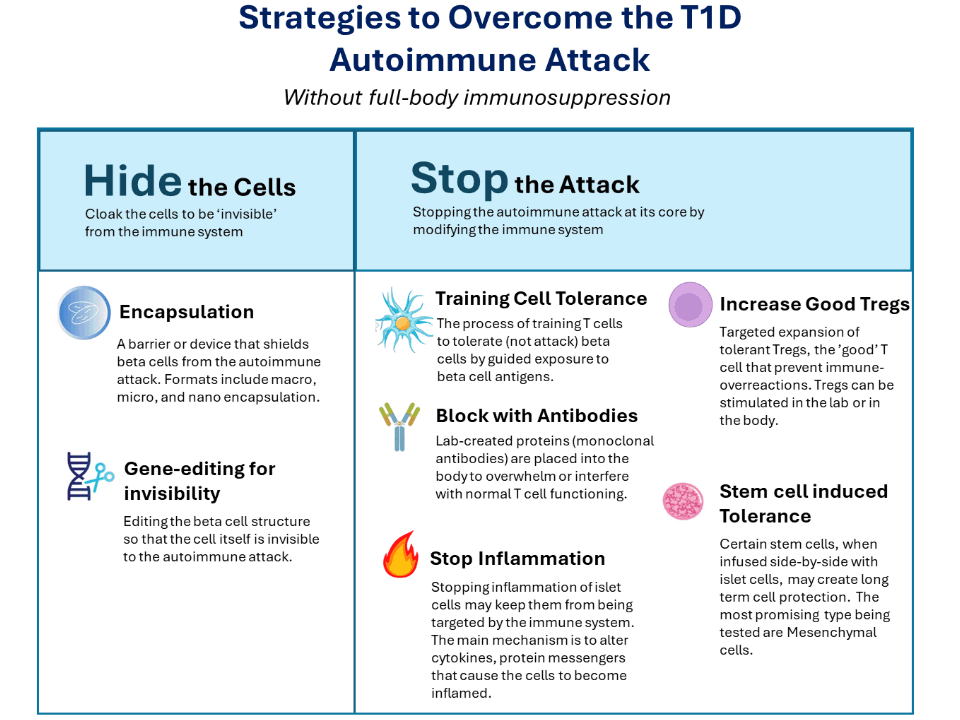
There are two major routes to overcoming the autoimmune attack, and several related research pathways:
- Hiding the Beta Cells from the immune system
- Stopping the Autoimmune Attack (at its root)
It is important to note that these pathways are still being developed and, accordingly, there are many unknowns. Any manipulation of the immune system, an incredibly complex apparatus, should not be taken lightly. A ‘good’ change to one aspect of this complex system may result in unintended bad side effects somewhere else. Each pathway and tactic will need to be fully vetted and tested for safety as well as effectiveness.
Hiding the Beta Cells
This route includes methods to hide beta cells from the immune system without altering it. Two primary research approaches are being explored:
1. Gene-Edited Cells
In this approach, the DNA of beta cells is edited to render them invisible to the immune system and/or trick the immune system into thinking they are not enemies. This capability to edit genes has evolved rapidly over the past decade and offers promise for advances in therapies for a wide range of diseases. While it is conceivable to edit genes either in the laboratory or in the body, the T1D research active today utilizes beta cells edited on the bench before transplantation.
In the Practical Cure trial UP421, led by Sana Biotherapeutics, gene-edited cadaveric islets were transplanted into an established T1D patient without chronic immunosuppression. The cells survived for fourteen months, a major breakthrough, even though not enough islets were transplanted to result in insulin independence.
The known risks of using gene-edited beta cells are, so far, limited to procedural discomfort or the antirejection drugs given beforehand (in some studies). But other potential risks have also been voiced. One concern is that if an invisible cell were to turn into cancer, the immune system would not defend against it. However, researchers are working on adding a genetic ‘safety switch’ to these cells, causing controlled cell death that only activates when exposed to a specific, otherwise safe drug.
2. Encapsulation
Islets are placed inside an encapsulation device, a physical barrier to hide them from autoimmune attack. All encapsulation devices have a semi-permeable surface designed to prevent immune cells from entering while allowing insulin to exit in response to blood glucose levels.
There are three primary types of encapsulation:
- Macroencapsulation: Many islets are placed in a singular device.
- Microencapsulation: A few islets are placed in each microcapsule.
- Nanoencapsulation: A singular islet is covered in a thin coating that clings to its shape.
There are several challenges in building a working encapsulation device. The device must not develop fibrosis (the formation of scar tissue) when implanted, which has been a major hurdle in early testing. It must ensure the beta cells get enough oxygen and blood flow, and it must be able to constantly read the body’s changing glucose levels.
Despite decades of development and testing in human trials, no encapsulation method has yet to prove effective (without using broad immunosuppression). However, new technological developments in biological materials and bioengineering keep this pathway in development.
Stopping the Autoimmune Attack
This pathway aims to stop the immune system from attacking insulin-producing cells by changing or interfering with the immune system at its root. Describing the approaches underway to stop the autoimmune attack is challenging in plain language. The science behind changing the immune system is complex and nuanced, with its own language and terms. We endeavor to keep descriptions as simple as possible while still credibly conveying the main points, but we openly acknowledge that, for clarity, we may miss some scientific nuances.
It is also important to note that any change to the immune system at its core raises the question of long-term, unknown, unintended side effects. We will share the adverse events known to date; we will not speculate on the longer term.
There are five approaches addressing this pathway:
1. Training Tolerance: Getting the Immune System to Accept Beta Cells
This approach aims to teach the immune system to tolerate insulin-producing beta cells without broadly weakening the rest of the immune system. The basic idea is like an allergy shot: repeated exposure may help the body learn not to overreact.
One strategy focuses on APCs, which act like teachers in the immune system. These cells help show T cells what to respond to and what to ignore. In this approach, researchers remove these immune cells from the body and train them in the lab to present beta-cell material in a way that encourages tolerance rather than attack. The cells are then returned to the body by IV.
The hope is that, once back in the body, these trained cells will help tell the immune system that beta cells should not be attacked. They may also encourage the development of regulatory T cells (Tregs) that help keep harmful autoimmune reactions under control. Over time, this could help the body become more tolerant of beta cells.
Today, this method is mainly applied to people with recently diagnosed type 1 diabetes who still have beta cells. In the future, researchers hope it could also become part of the treatment for people with established T1D.
Known risks may include flu-like symptoms, infusion-related reactions, and other immune effects that are still being studied.
2. Blocking the Attack with Antibodies
Lab-created proteins called monoclonal antibodies are put into the body to interfere with and overwhelm normal T-cell function, specifically regarding beta cells. The hope is that this interference will render the T-cells unable to launch or complete the autoimmune attack.
This works by creating special lab-made proteins that target and bind to specific immune cells. Once bound, there are three different interference actions that researchers are exploring: (1) interrupting the ‘conversation’ that occurs between immune cells and beta cells to stop the attack; (2) exhausting T cells so they are too tired to activate; or (3) depleting cells that coordinate the immune response.
This approach is being explored in numerous clinical trials. A high-profile example is Sanofi’s Tzield, though this is not a Practical Cure.
Primary patient risks known today include infusion reactions, drops in white blood cell counts, increased infection risk, and potential for immune-wide adverse effects.
3. Stop Inflammation
The main idea behind this pathway is that by suppressing inflammation in islet cells, we can effectively halt the autoimmune attack. In T1D, islets are chronically inflamed, causing blood vessels to widen, allowing more attacking immune cells to reach beta cells in the pancreas. If we can stop this process, we might be able to keep beta cells alive and allow them to thrive.
One approach is to block the activity of certain inflammatory proteins called cytokines. In T1D, cytokines released by immune cells can bind to beta cells, triggering stress while amplifying inflammation and recruiting T cells for the attack. As a result, beta cells can become more stressed, more dysfunctional, and more vulnerable.
To block the cytokines from inducing inflammation, scientists are testing several different approaches. These methods include introducing specific antibodies into the body to stop pro-inflammatory cytokines, and/or transplanting cells that produce anti-inflammatory cytokines.
The risk to patients could be significant. Because of cytokines' role in regulating the overall immune system, this method could impact overall immune function and increase the risk of infections. Efforts to mitigate this include targeted delivery, dose escalation, and patient monitoring/prescreening.
4. Increasing the Amount of Regulatory Tregs
The goal of this approach is to increase the number of healthy Tregs to prevent the autoimmune attack in type 1 diabetes. Tregs are a special type of T cell, often called the ‘bodyguard’ of the immune system. Their job is to stop the immune system from mistakenly attacking the body’s own healthy cells.
Researchers are testing different ways to increase or strengthen Tregs. One method uses substances such as cytokines or antibodies to encourage the body to make or support more Tregs. Another involves taking immune cells from a patient, turning or expanding them into Tregs in the lab, and then infusing them back into the body.
Researchers are also exploring gene-edited Tregs, often called CAR-Tregs. These cells are modified to more precisely target the harmful immune response, with the aim of better protecting beta cells.
Possible risks include infusion reactions, unintended immune effects, and excessive immune suppression. Another concern is that some cells may not remain stable or function as intended after infusion. Newer approaches, including gene editing and the use of a patient’s own cells, are in development to improve precision and reduce these risks.
5. Stem Cell-Induced Tolerance
The goal of this approach is to protect newly transplanted beta cells by infusing supportive stem cells alongside them. The theory is that these added cells could help create a safer, more supportive environment as the beta cells settle into the body.
The stem cells most often discussed for this role are mesenchymal stem/stromal cells (MSCs). Researchers believe MSCs may help by calming inflammation, reducing the immune attack, supporting tissue repair, and helping transplanted cells establish a healthier blood supply. In simple terms, the hope is that the beta cells would be transplanted with a built-in support team.
This idea is promising, but it is primarily tested in early-onset T1D. Scientists do not yet know whether supportive stem cells alone can provide enough protection to stop the autoimmune attack in established type 1 diabetes over the long term. Many researchers believe this approach may need to be combined with other protective strategies, such as immune therapies, gene editing, or encapsulation devices.
Possible risks of MSC-based approaches include infusion reactions, nausea, fever, pain at the infusion site, and, in rare cases, blood clots or fibrosis. Researchers are continuing to study how to make this approach safer, more reliable, and more targeted.
A separate and more intensive stem-cell-based approach uses blood-forming stem cells to try to “reset” the immune system. The risks of this treatment are different and can be more serious, as it requires a ‘clean’ slate before transplant, meaning the immune system is wiped out via chemotherapy or another pre-transplant regimen beforehand.