
This report opens with the uncomfortable fact that the type one diabetes (T1D) research and fundraising ecosystem is not set up to achieve a Practical Cure in the next 15 years. No Practical Cure projects have yet progressed beyond Phase-II clinical trials and money for cure-focused research spending fell to historic lows at the major grant-giving organizations this year. The four recommendations below provide a blueprint for researchers, fundraisers, and donors to align with the goal of achieving a Practical Cure for T1D.
1. Nonprofits, medical researchers and donors should adopt a standardized Practical Cure definition.
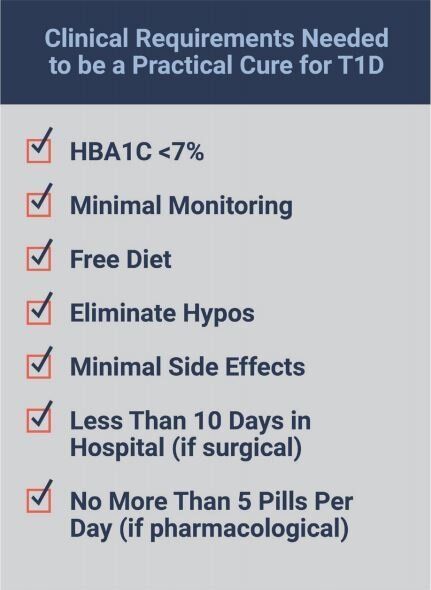
Before funds and resources can be allocated towards a Practical Cure, this objective must be clearly defined and established. The graphic shows the clinical requirements a Practical Cure solution would achieve and adhere to. Although a Practical Cure does not constitute a full reversal of the disease, it would deliver a dramatically improved and 'near-normal' quality of life for 1.25 million Americans living with type one diabetes and substantially reducing the financial, emotional, and medical burden of the disease. Research and funding should be oriented towards this goal.
In addition to the clinical requirements, any Practical Cure solution must be available to market within the next 15 years. There are two essential benefits to structuring the goal within such a timeframe. First and foremost, we must deliver a solution that can transform the lives of people living with the disease today. Second, a 15-year timeline provides a structure for prioritizing projects. The JDCA believes that projects that have already advanced into human trials should be given priority, fully funded, and wholly resourced so they can move through those trials to conclusive results as quickly as possible. In our view, projects that will not be available in the next 15 years should receive lower priority in terms of research funding. Successful or not, late-stage Practical Cure projects should be brought to a conclusion as quickly as possible.
2. T1D researchers and executives should be incentivized to achieve a Practical Cure in 15 years.
Once a Practical Cure definition with a 15-year timetable has been accepted, the major T1D nonprofits and government organizations need to become more proactive in soliciting Practical Cure projects. The JDRF, ADA, NIH, and CDC should identify Practical Cure research as a core area of focus. This would fundamentally change the relationship between these grant-giving organizations and the research community. Ample funding and recognition for Practical Cure breakthroughs would finally incentivize and encourage T1D researchers to design and pursue Practical Cure projects.
Furthermore, salary incentives must be used to encourage nonprofit leaders and research investigators to pursue a Practical Cure vigorously. Nonprofit CEOs, principal investigators, and the staff within these organizations should see their workflow, performance expectations, and incentives aligned with finding a Practical Cure in the next 15 years. In 2018, ADA and JDRF executives were paid most of their compensation regardless of whether they met their main objectives or made progress toward a cure for T1D. This differs from the dominant model which guides for-profit companies' executive salaries as well as that of a handful of successful non-profits. The American Heart Association (AHA), for instance, uses metrics and goals related to both fundraising and mission goal progress to incentivize executives. In 2018, 46% of the American Heart Association’s CEO compensation was tied to performance.
The JDCA has written extensively on how to tie T1D nonprofit executives to Practical Cure performance in our annual executive compensation report. (click here to read).
3. JDRF and ADA should restore cure-focused funding from historic lows.
In 2018, JDRF spent only 37 cents of every dollar raised funding research, almost 50 percent less than their rate ten years ago. Of that, only seven cents were used to specifically fund cure research. Meanwhile, the ADA spent only $3.8 million (out of $161 million raised) specifically on T1D research in 2018, a 10-year low. This decline must be stopped if there is to be a real chance for a Practical Cure in the next 15 years.
To date, neither organization has adopted a Practical Cure initiative as one of the main parts of its research portfolio. However, if adopted, we have no doubt they have the ability, experience, and resources to make progress quickly towards curing type one Diabetes for people who have the disease today. In our assessment, no other organizations are as well-positioned to make great strides towards a Practical Cure as the ADA and JDRF.
4. Donors should take action directed at Practical Cure research funding.
Financial donors also play a key role in ensuring that a Practical Cure research platform is a top priority. As the primary source of income for the main diabetes charities, donors have the right to voice their point of view. Without ongoing pressure from donors to adopt, institutionalize, fund, and fully resource Practical Cure research, it is unlikely this outcome will be achieved in the next 15 years. We encourage donors to do their part by speaking up:
- First, donors should voice their interest in a Practical Cure initiative at local fundraising events by letting their local chapter heads know about their interest in Practical Cure research by contacting the ADA and JDRF headquarters to make their voice heard.
- Second, we encourage you to contact JDRF's CEO, Aaron Kowalski on twitter @aaronjkowalski, by addressing an email to him at info@jdrf.org, or by calling JDRF at 212-785-9595 and expressing your interest in a Practical Cure research initiative.
- Third, when you make a donation, we recommend that you include a written request that the money is used for cure research. The receiver is obligated to use the donation as you wish.